Well, now we know what it takes to get me to write a new blog post: The gentlest threat of legal action I've ever received!
I mean, compare and contrast the start of the Firepower debacle, or these guys, with this genteel and civilised missive.
From: Andy McCutcheon <Andy.McCutcheon@niagara.com.au>
Date: Tue, 19 Jan 2016 02:19:26 +0000
To: "dan@dansdata.com" <dan@dansdata.com>
Subject: Blog PostHi Dan;
I have enjoyed reading several of your blogs - you have a naturally cynical humour much the same as mine!
I am the recently appointed Head of Digital for CT Healthcare Global, who owns Niagara Therapy, Equissage and Accell Therapy. As such I have been made aware recently of a number of subjective blog posts on numerous sites that in many cases start off innocently, but tend to attract commentary that is full of misinformation, untruths and borderline libellous information about the company. Many blog posts are un-moderated and therefore are allowed to fester. Since many blogs continually pump fresh content they index very well on search engines and therein lies the issues.
The post on your site which was done back in 2012 is somewhat accurate and at the time, the company was finding flyer distribution a viable means of generating interest in their products. In the past twelve months however and more specifically when I took over in October, I have made sweeping reforms to the way that data is collected and the type of data that is presented in the marketplace.
I have been busy consolidating a new website (This is a link to the staging site) http://www.gcwebdesign.com.au/niagara.com.au/ [if you're reading this long after I posted it, in due course the staging site will presumably become the new niagara.com.au] to include all of their brands and culling a tremendous amount of superfluous content that is not required, removing information on medical terminology or outlandish sounding medical claims. Having said that, being highly regulated by the TGA we are closely governed by the Australian Government in both our ISO manufacturing processes as well as our conscionable code of conduct.
While much of the commentary is somewhat accurate - it is also quite misleading. The form you have posted has not been accurate since 2013 and on that basis I was wondering if you wouldn't mind taking the thread down for no other reason than inciting subjective commentary based on outdated information?
I am more than happy to assist you in posting accurate information about the company if you wish to do so or since you are in Australia free to come to the HQ for a tour so you can see first-hand what we do and what our medical devices do and how they have helped millions of people since 1949?
Can you please come back to me on this?
Regards
Andy McCutcheon
Head of Digital Marketing
Australia & New ZealandMob: +61 401 780 488 Tel: +61 7 3386 7256 NZ: 0800 55 2526
Address: 29 Resource Street, Parkinson Q 4115. PO Box 698 Archerfield Qld 4108
Email: andy.mccutcheon@niagara.com.au
www.niagara.com.au
www.equissage.com.au
www.accelltherapy.com.au
Seriously, I'm impressed. This is the way to do it, guys.
(Oh, and yes, it took me more than a week to even notice he'd sent me this. So it goes.)
Of course, Andy, I'm not going to take that blog post down. The gentleness of your language makes clear, I hope, that you know that actual legal threats would be ridiculous in this situation, if I have good faith, public interest and truth on my side. I remind you that defamation law in Australia was relatively recently changed to make truth alone a sufficient defence against a libel action. While you make reference to "misinformation" and "untruths", you seem to have neglected to actually name any such things I have written. Without such specific complaints, you seem to me to just be unhappy about people's expression of their opinions based on disclosed information. Suing critics for this reason is popular, but wrong.
That previous post had three main points.
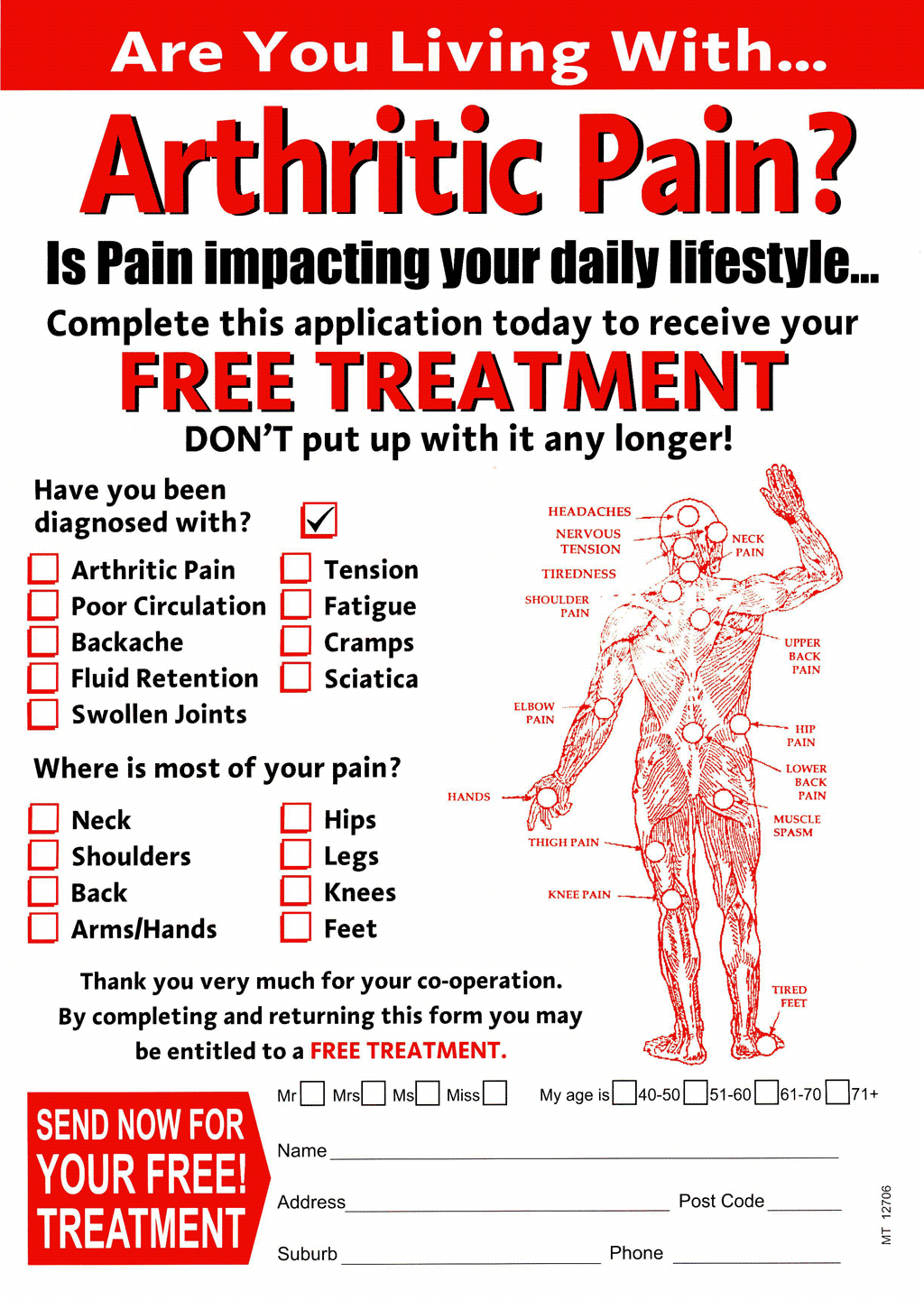
One, I got a really impressive piece of junk mail from Niagara, except they didn't even admit what their name was on the junk-mail. Which, as you say, was probably not a good policy, and I'm glad you're changing it.
Two, Niagara not only concealed their name, but also kept their prices a secret. This seems to be because the prices are really, really high, and you don't want to scare off customers with a price tag before you can explain the many excellent qualities of your products which make them well worth the money.
Three, Niagara have, as you say, been in business for an awfully long time, but have in that time found it difficult to take a moment to prove that their products actually are better than many far cheaper massage-y things.
That's really the clincher. Like the makers of a zillion other odd health products, Niagara said they had scientific evidence that their products were worth buying, but that evidence was actually... scant.
I wrote about that evidence at the time, in some detail, and I must note once more that despite your stated concerns about "untruths" you have not actually mentioned anything in my 2012 post, or even in the comments, that is wrong - only that it doesn't reflect the state of Niagara's operation today.
I am happy to write this new post, therefore, and will add a link to it from the old one. Glad to be of service!
The core of the whole thing remains the evidence, so let's check out the new and improved Niagara Medical Research pages (which I presume will in due course move to here.)
I downloaded the 15 documents currently available on the two Medical Research pages. Many of them actually are published medical studies, or a review of groups of studies. So that's a good start. Some of this is stuff I talked about in the last post, but because my only real function in the world is processing information and attending to the needs of five cats, I read everything again and will write anew about it here.
In no particular order, I started my reading with "Influence of Cycloid Vibration Massage on Trunk Flexion".
("Cycloid Vibration" is Niagara's unique selling point, a multi-dimensional mechanical massage system that is alleged to be sufficiently superior to, say, your standard Sharper Image massage chair, to justify prices that make the Sharper Image chair's price look reasonable for the first time in human history.)
This study is from 1960; Niagara's evidentiary documents are in general not terribly new. If something worked in 1960 then it'll still work now, of course, so let's press on.
It tests the effect of "cycloid massage" on trunk flexion, in a respectable sample of... healthy people. There is, however, some kind of control; some of the subjects just laid down quietly with no massage, which actually by itself seemed to slightly help trunk flexibility.
More importantly, however, and I'm afraid I'm going to be saying this rather a lot of times in this post, this study made no test of a simple vibrating massager versus a fancy "cycloid" one.
And, in any case, even if cycloid massage was simply brilliant at increasing the trunk flexibility of healthy people, and even if it's better than a cheap massager, that doesn't prove anything about the claims being made to actually sell the Niagara products, which are not marketed to healthy people who'd like to be able to bend over slightly more.
OK, on to "Joint mobility changes due to low frequency vibration and stretching exercise". This one's from 1976. Abstract: "It has been shown that fifteen minutes of locally applied cycloid vibration of low amplitude and frequency is equally as effective as a fifteen minute programme of flexibility exercises in increasing short term mobility of the hip flexors."
Again, the people being tested were not sick - "Forty-two healthy young adult males", the same kind of university undergrads that show up in so many, many studies, for obvious reasons. There was again at least a partial control, because this was a crossover study - the control "treatment" was just sitting quietly in a chair, but every participant got the massage, and did the stretching exercises, and did the "control", just on different days.
This study found effects as per the abstract. But did they test a simple vibrating massager against a cycloid device? No. And did they get any information relevant to Niagara's core pain-reduction and illness-treatment claims? Also, so far as I can see, no.
OK, on we go to "Results of a large scale clinical trial of the Niagara Thermo Cyclopad®", which is a substantial document that does speak to one of the Niagara sales claims - treatment of lymphoedema. It's also quite recent, having been done in 2001. It's never been published in a peer-reviewed journal, though, and its two primary authors aren't exactly monsters of academic publishing.
(Here's the first primary author's current two lonely Medline hits. I suspect the "Judith H Merritt" to be found in the author listings for a decent number of published papers is not the same as the "Ms Judith Merritt" co-authoring the Niagara paper, however, because Judith H. Merritt doesn't seem to deal with many study subjects large enough to see with the naked eye.)
None of this should be taken to mean that I think the Thermo Cyclopad® report is slanted research-for-hire, but given the plethora of extremely implausible and indeed mutually contradictory devices that use as their evidence a great big "scientific study" that was never published and was written by unknowns, I think I'd be remiss not to mention these details.
(Please note that I also try to carefully and consciously control my own unfair propensity to disbelieve any scientific study with a registered-trade-mark symbol somewhere in its title.)
Aaaaaanyway, in the Thermo Cyclopad® study there is another odd-sort-of-control, that being 20 "normal" people who did not have lymphoedema, using the Niagara massager to "determine if the normal population could gain some benefit".
In this normal-participants section of the study, the massagey-thing reduced leg volume a bit, but only in the subjects' left legs. Not the right.
I think you'll find that anybody who's done science and stats can tell you that a result like this is a classic indicator that you're measuring nothing. So far as I can see, the rest of the normal-participant results, all faithfully graphed, bear out this interpretation. Various things changed a little bit, some in a direction that'd be good if these subjects actually had lymphoedema, others in directions that wouldn't be.
I think my favourite "evidence of absence" result in the normal-subjects tests is that apparently three weeks of massage-pad use reduced the subjects' heart rate by 6%.
Some basic health indicators - weight, BMI, that kind of thing - moved in healthy-looking directions in the "normal" cohort, but I'd venture that just knowing you're in a "medical study" of some kind may encourage you to walk a bit more and eat fewer burgers. Researchers try to control for this, but unless you keep all your study subjects locked up in a panopticon, you can never perfectly keep up with their behaviour.
Okay, who cares about that first part of the study, those people were already fine, it didn't hurt to buzz 'em about a bit and see if anything happened. What about the subjects who actually have lymphoedema?
Well, there are plenty of graphs in the, deep breath, "secondary lymphoedema and primary lymphoedema or mixed primary and secondary lymphoedema participants" section. The first of those graphs, of leg volume - the measurement that was so weird with the "normal" cohort - is pretty good. And left and right legs changed in the same way, which was no doubt good news for the sanity of the researchers.
Not much actually happened to the lymphoedema subjects' leg volume during the treatment period, but the follow-up four weeks later showed a considerable leg-volume reduction, suggesting that some kind of structural improvement may have happened.
(Or, once again, the participants may have tended to do some other thing that helped with their leg volume, like for instance getting a prescription for diuretics, or bandaging, or exercise. And again, having been part of a study may have changed their behaviour in other ways. The study says it controlled for this and the statistically-significant results still stood... but patients forget. And lie.)
All the rest of the graphs in this section are pretty much flat. Overall they slope a teeny bit in a promising direction - blood pressure is the best of these, but blood pressure isn't what this study is supposed to be about; measure enough things and you're guaranteed to find something you can spin as news. But, overall, not much of anything actually changed.
On to the Venous Oedema section. It starts with "No statistically significant results were obtained for this group", so I shortened my workday by zipping right on by to "Lipoedema participants", who were also bereft of statistically-significant results and thus saved me from poring over numerous further pages.
(This, by the way, is excellent evidence for this not being a work-for-hire fake study. If you're paying people to say your product is great, they may not write a transparent work of banana-republic election propaganda that says 144% of the vote went to the President-For-Life, but they also won't start whole chapters of the report with, "um, well, perhaps the patients felt better, but we certainly couldn't measure it!")
On to "Lymphatic function". This might have been helped a weeny bit, but had a sample size of only five, so who can tell.
Then there are the subjective quality-of-life reports, in which about half of the cohort reckoned the massage treatment helped them in one or more areas. Good for them. (A few also reported some peculiar unpleasant side effects. Generally speaking, both positive and negative subjective reports from medical-study participants are likely to be poor-quality data.)
Then there are Case Studies looking in more detail at things already reported, and then the Conclusions, which do their best to make the Thermo Cyclopad(R) look good... "from a holistic point of view".
Overall, I'd say this whole 94-page study probably looks great all leather-bound and sitting on Niagara's "Clinical Evidence" shelf, but if you actually read it, it's severely underwhelming. Not least because, yet again, they tested the expensive Niagara massager but not against a cheap one.
Next document!
Now we've got "The Influence of C.V.T. on Muscle Spasm", a paper that was "read at the 33rd session of the American Congress of Physical Medicine", et cetera et cetera, "1955", if you can believe that. It makes various claims about the benefits of "cyclotherapy" (which, by the way, is also a term for some kind of cancer treatment unassociated with Niagara), not the least of which is that it was reported to reduce "spasticity in a large percentage" of multiple sclerosis patients.
The source of this information?
A "personal communication" from a doctor in Pennsylvania.
And there are various other case reports and testimonials, and the conclusion that cycloid vibration "possesses that advantage of relative innocuousness, of simplicity of use, and of ready availability", but of course nothing about even more readily available cheap vibrating massagers.
OK, what about "The Influence of C.V.T. on Physical Activity"? Streaking forward in time to the Space Age year of 1961, it studies "normal college students ... in good physical condition", and "nearly all of the subjects in the treated group served as controls but on different days" - so, another crossover study.
It found the massager could cause muscle relaxation, which was probably not news even in 1961. The researchers found the time to test four different kinds of "cyclo massage" to really nail down the certainty of this finding, but once again it somehow slipped their mind that they ought to try other kinds of massager as well. And maybe even do a blinded test where the people doing the massaging don't know that one thing they're using or lying on or sitting in is the Special Niagara Massager That We're Pretty Proud Of Don't You Know, and another is a Boring Vibrator That Probably Came From One Of Those "Sex Shops" And Is Probably All Sticky Eww.
Ahem.
Right, on we go. "The Influence of Vibration on Temperature and on the Clearance of Radioactive Sodium in Human Subjects".
A study from Nineteen Fifty Frickin' Six this time! A study done on people who were actually sick! A study that showed that the special cyclo vibraty thing warmed people up a bit! A study that found that fluid injected into skin or muscle (not blood vessels) probably dissipated into the body faster when the body was buzzed! A study that, once more, did not test the cyclo-thingy against normal vibrators!
"Changes in the Pattern of Breathing Caused by Chest Vibration", from 1976. Unconscious cats and rabbits breathed ten to fifteen per cent more deeply when being buzzed. Might be relevant for things like asthma and sleep apnoea, I suppose, except then they went on to try it on six humans and it didn't do anything - well, not anything good. Study observes that effects on respiration from vibration had been found in several other studies. Says nothing about why you'd particularly want a Niagara vibrator for this purpose. Particularly given that it didn't seem to work.
"Effect of Chest Vibration in Pulomonary Emphysema". A "preliminary report" from 1968, and this PDF is a really terrible facsimile of it, but the full text unfortunately doesn't seem to be online anywhere.
Refers to other studies already mentioned, puts a rather small sample of obstructive-lung-disease patients in a couple of different versions of buzzy chair, discovers that they breathe slower but deeper when being buzzed. Minute volume - total volume of gas breathed per minute - fell. Apparently this is a good thing. Non-fancy vibrating chair not tested. Theorises that "the feeling of relaxation induced by this procedure appeared to be the important factor..." for one sub-sample of subjects. Does not wonder whether a massage chair from SkyMall or something wouldn't be just as relaxing. I suppose they didn't have SkyMall in 1976.
Aaaand then there are a couple of literature reviews.
One is all about whether it's safe to use electronic massagers when you've got a pacemaker. OK, whatever.
The other literature review mentions some of the above, plus a few studies that aren't on the Medical Research page.
In the part at the beginning talking about how they searched for the papers and the things they excluded from the search, this literature review alerted me to the existence of something called "ejaculation therapy". Not "premature ejaculation therapy", just "ejaculation therapy". Well, if it feels good, do it, that's what I say.
Ahem, once again.
According to the review, those other studies said:
In 1981, mice healed faster and better when cycloid-vibrated. Cheap vibrator not tested.
In 1984, 16 old ladies with crook knees reckoned that Niagara was better than nothing. Niagara not tested against cheap vibrator. (At least one of the old ladies probably could have loaned the researchers a cheap vibrator. I'm just saying.)
Tissue fluid drainage in presumably rather confused pigs with no superficial lymph nodes. Niagara helped. No cheap-vibrator test.
A "high quality controlled single blind crossover human study" of Niagara against "current best practices" in tissue-fluid-drainage, and and Niagara looked pretty good, but they didn't test... by now you'll know how that sentence ends.
Oh, and in a follow-up after a month with no Niagara-ing, this study found that limb volumes had returned to what they were, contradicting the big 2001 study mentioned above.
More people seeking medical help in the movement of unwanted bodily fluids. Again Niagara seemed to work well, in objective measurements and quality-of-life reports. Again no cheap-alternative comparison.
In 1976, buzzing people's hands increased skin blood flow. No cheap comparison.
In 1984, buzzing reduced blood pressure a bit. No cheap comparison.
But in 2006, people with orthostatic hypotension - undesirable reduction of blood pressure when sitting quietly - had their problem suppressed by buzzing.
Buzzing! It's good for what ails you! But there was no comparison with a cheap alternative!
Also on the Medical Research pages are three Register of Therapeutic Goods certificates proclaiming that Niagara products are legal to sell in Australia. There's also an ISO certificate verifying that whatever it is that Niagara does, they manage and document these activities to ISO 13485 standards.
And then there's a pamphlet about THE CYCLOID VIBRATION PRINCIPLE, which makes various assertions about, for instance, the "superb results" Niagara's special vibrators have had in the treatment of edema.
Only the CYCLOID ET CETERA pamphlet, among these last five things, even loosely resembles "Medical Research". The others should not be on the Medical Research page. Far be it from me to suggest that perhaps their role is to pad out this online version of the abovementioned Clinical Evidence shelf.
And that's the end of Niagara's evidence.
So. Andy. Mister McCutcheon. Maaaaate.
I have spent six hours reading through this stuff and writing this post, and I am confident in saying that it has absolutely one hundred per cent confirmed what I said before.
Niagara's alarmingly expensive buzzy things may be good for this or that, but people who do studies of Cycloid Vibrational Thingummies, which as you so proudly say has been an area of study for sixty years now, mysteriously never, never, never test Niagara products against cheap alternatives.
I find it very difficult not to consider this something of a red flag.
Your new Web site, like the current one, has a Products page. Let's just look up the prices then, shall we?
The secret pricing of Niagara products was, you'll recall, a big part of the reason why my previous post was less than entirely, well, sold on your ideas.
Wow, you've got "Customised Pricing Solutions For Every Budget"!
That's great!
I didn't put the quote marks around that statement, though, they're there already on the Web page as I write this. But never mind that supercilious feeling I get when I see a sign promoting "Fresh" fish or "Delicious" sandwiches, I'm sure you're sincere. Let's just-
"We Have A Number Of Tailored Payment Solutions We Can Offer Starting At Only AUD$15.00 per week."
Aaaand... that's it for the pricing information, so far as I can see.
Potential customers can, on the current site or your new one, not see what your products will actually cost them, but only request a quote.
Which I presume, as before, will be delivered by a Niagara employee earnestly seeking to make a sale.
And if the customer is advanced in years and limited in means, I am sure that Niagara, with its much-vaunted long commercial history, is entirely willing to patiently relieve said customer of the mere $AU780 per year which the minimum payment entails, until in due course Niagara is made entirely whole when the balance of the principal-plus-interest is paid by the customer's estate.
Sigh.
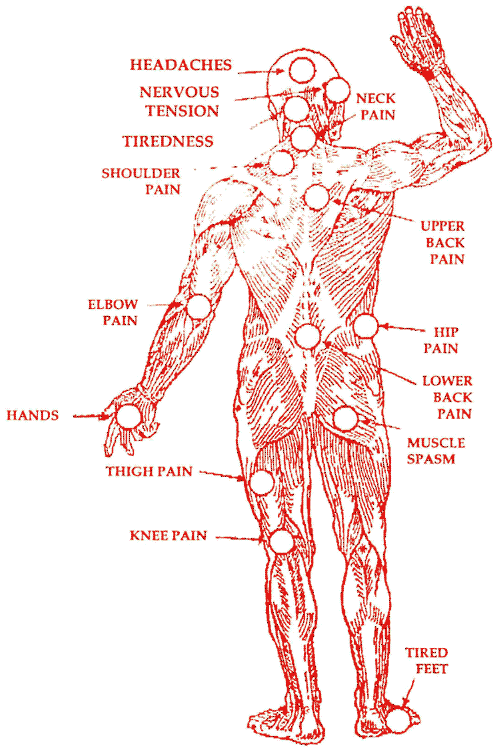
Oh, by the way - are you still presenting potential customers, by the nature of the kind of relief you promise tending toward the old and dotty end of the skepticism spectrum, with anatomical diagrams where pain in the customer's anything will surely be eased by a Niagara product of unknown price-tag?
Are you still putting those diagrams on junk-mail and shooting outrageous amounts of said junk-mail all over the world?
Well, I presume you are telling the truth when you say that you aren't. Good for you. Woo.
But no, Andy, I am not going to take down a post about what an organisation did in the past because it promises not to do those things in the future. Especially when it is demonstrably still doing every one of those things that matters.
I believe our brief correspondence can here be ended.
[UPDATE: A day after this went up, Andy McCutcheon replied to the insolently-courteous e-mail I sent him to tell him I'd not done what he asked, and had instead just talked about the concerns I had about Niagara products at much greater length than before.
His response was,
Much better. Thanks
Succinct. But, again, much more courteous than I've come to expect from people who get upset about my writings.]